Article:
Mental retardation is one of the most common childhood pathologies. About 50% of all low-achieving schoolchildren are diagnosed with this condition. Moreover, most of them study in regular general education schools, not correctional schools, despite the fact that they are not able to master the knowledge provided for in traditional programs. As a result, a lot of problems arise for teachers (how to teach) and parents (how to develop). In fact, mental retardation in children is not a death sentence at all. Competent and regular classes are a guarantee of successful psychocorrection work.
What it is
Mental retardation is a mental retardation when the basic cognitive functions (thinking, memory, attention, emotional-volitional sphere) in a child are not as well developed as those of peers and differ from the norms established for a given age. Diagnosed only in children of preschool age or primary school. If signs of the disease remain at the time of transition to secondary care, more serious diagnoses are made - for example, constitutional infantilism or mental retardation.
The term was proposed by the Soviet psychiatrist G. E. Sukhareva in 1959. Widely used in psychological, pedagogical and medical practice and literature. However, at the end of the 90s of the 20th century it was considered too generalized and already outdated, so the question of its replacement was raised. In 1997, this diagnosis was withdrawn from use by order of the Ministry of Health. They have been replaced by new concepts corresponding to codes F80–F89 and F90–F98 in ICD-10. These include all kinds of psychological development disorders (but no longer mental disorders):
- expressive and receptive speech disorders;
- hyperkinetic disorders;
- dyslexia;
- dyscalculia;
- dyspraxia;
- dysgraphia;
- behavioral disorders;
- phobias;
- tics;
- enuresis;
- encopresis;
- stuttering.
Since 1997, the term is not applicable as a medical diagnosis and is not opposed to mental disorders. However, this concept continues to be widely used in Russian-language psychological and pedagogical literature and Russian educational institutions.
Mental development delays in children and principles of their correction (review)
The mental development of a child is a complex, genetically determined process of sequential maturation of higher mental functions, realized under the influence of various environmental factors. The main mental functions include: gnosis (recognition, perception), praxis (purposeful actions), speech, memory, reading, writing, counting, attention, thinking (analytical and synthetic activity, the ability to compare and classify, generalize), emotions, will, behavior, self-esteem, etc.
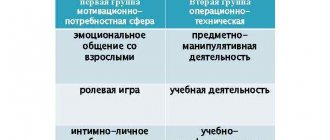
V.V. Lebedinsky (2003) identifies six main types of mental development disorders in children:
- Irreversible mental underdevelopment (oligophrenia).
- Delayed mental development (reversible - fully or partially).
- Damaged mental development - dementia (the presence of a previous period of normal mental development).
- Deficient development (in conditions of visual impairment, hearing impairment, somatic pathology).
- Distorted mental development (early childhood autism).
- Disharmonious mental development (psychopathy).
Mental development delays in children and their correction are an urgent problem in pediatric psychoneurology. The term “mental retardation” was proposed by G. E. Sukhareva back in 1959. Mental retardation (MDD) is understood as a slowdown in the normal rate of mental maturation compared to accepted age norms. ZPD begins in early childhood without a previous period of normal development, is characterized by a stable course (without remissions and relapses, unlike mental disorders) and a tendency to progressive leveling as the child grows older. You can talk about mental retardation until primary school age. Persistent signs of underdevelopment of mental functions at an older age indicate oligophrenia (mental retardation).
Conditions classified as mental retardation are part of the broader concept of “borderline intellectual disability” (Kovalev V.V., 1973). In the Anglo-American literature, borderline intellectual disability is partly described within the framework of the clinically undifferentiated syndrome “minimal brain dysfunction” (MMD).
The prevalence of mental development delays among the child population (as an independent group of conditions) is 1%, 2% and 8–10% in the general structure of mental illnesses (Kuznetsova L. M.). Mental development delays as a syndrome are naturally much more common.
The pathogenesis of ZPR is poorly understood. According to Pevser (1966), the main mechanism of mental retardation is a violation of maturation and functional failure of younger and more complex brain systems, related mainly to the frontal regions of the cerebral cortex, which ensure the implementation of creative acts of human behavior and activity. There are currently no uniform forms of systematically borderline forms of intellectual disability. The most detailed classification of borderline states of intellectual disability presented by V. V. Kovalev (1973).
There is a division of ZPR into primary and secondary. In this case, secondary mental retardation occurs against the background of a primary intact brain in chronic somatic diseases (heart defects, etc.) accompanied by cerebral insufficiency.
In the first years of life, due to the immaturity of the nervous system, children often experience dysfunction in the maturation of motor and general mental functions. Therefore, usually in early childhood we are talking about a general delay in psychomotor development with a greater severity of mental function lag.
In children over three years of age, it becomes possible to identify more defined psychoneurological syndromes. The main clinical signs of mental retardation (according to M. Sh. Vrono) are: delayed development of basic psychophysical functions (motor skills, speech, social behavior); emotional immaturity; uneven development of individual mental functions; functional, reversible nature of the disorders.
If intellectual disability in preschool age is masked by speech disorders, then at school age it manifests itself clearly and is expressed in a poor supply of information about the environment, the slow formation of concepts about the shape and size of objects, difficulties in counting, retelling what has been read, and a lack of understanding of the hidden meaning of simple stories. In such children, a concrete-figurative type of thinking predominates. Mental processes are inert. Exhaustion and satiety are expressed. The behavior is immature. The level of visual-figurative thinking is quite high, but the abstract-logical level of thinking, inextricably linked with inner speech, turns out to be insufficient.
V.V. Kovalev distinguishes intellectual disability resulting from defects in analyzers and sensory organs in cerebral palsy and early childhood autism syndrome as separate forms of intellectual disability.
ZPR syndrome is polyetiological, the main reasons are:
1) perinatal lesions of the central nervous system (hypoxic-ischemic, traumatic, infectious, metabolic; alcohol and other fetopathies); 2) epilepsy and epileptic encephalopathies; 3) hydrocephalus (including hyporesorptive disorders); 4) craniostenosis; 5) brain tumors; 6) malformations of the brain (dysgenesis of the corpus callosum, holoprosencephaly, arachnoid cysts, etc.); 7) hereditary diseases (phenylketonuria, histidinemia, homocystinuria, etc.); mitochondrial diseases; 9) storage diseases; 10) chromosomal diseases (Down syndrome, fragile X chromosome, etc.); 11) hereditary syndromes; 12) neurocutaneous syndromes (neurofibromatosis, tuberous sclerosis, encephalotrigeminal angiomatosis, etc.); 13) congenital endocrine diseases (congenital hypothyroidism, etc.); 14) autistic disorders (Kahner's syndrome, Asperger's, Rett's syndrome, etc.); 15) somatic pathology (heart disease, kidney disease, etc.); 16) decreased visual and auditory function; 17) pedagogical neglect.
2) epilepsy and epileptic encephalopathies; 3) hydrocephalus (including hyporesorptive disorders); 4) craniostenosis; 5) brain tumors; 6) malformations of the brain (dysgenesis of the corpus callosum, holoprosencephaly, arachnoid cysts, etc.); 7) hereditary diseases (phenylketonuria, histidinemia, homocystinuria, etc.); mitochondrial diseases; 9) storage diseases; 10) chromosomal diseases (Down syndrome, fragile X chromosome, etc.); 11) hereditary syndromes; 12) neurocutaneous syndromes (neurofibromatosis, tuberous sclerosis, encephalotrigeminal angiomatosis, etc.); 13) congenital endocrine diseases (congenital hypothyroidism, etc.); 14) autistic disorders (Kahner's syndrome, Asperger's, Rett's syndrome, etc.); 15) somatic pathology (heart disease, kidney disease, etc.); 16) decreased visual and auditory function; 17) pedagogical neglect.
Over the course of the last decade, a natural connection between cognitive developmental disorders and epilepsy and epileptic activity in the brain has been identified. Epileptiform discharges in the EEG are quite widely observed in individuals who have never had epileptic seizures. Uncontrolled spread of spontaneous epileptic discharges with cascade-like involvement of potentially normal neurons in pathological synchronization outside of seizures leads to their inability to perform normal functions, which is manifested by the entire spectrum of cognitive disorders.
According to many studies, epileptiform activity is observed in the EEG of patients with cognitive impairment from 20% to 90%, depending on the form of pathology. Thus, a large area of overlap between mental development disorders and phenotypes with epileptiform and epileptic activity in the EEG has been identified. Accordingly, the Working Group on Classification and Terminology of the International League Against Epilepsy introduced the heading “Epileptic encephalopathies” into the draft new classification of epileptic syndromes, which includes epilepsies and epileptic syndromes in which epileptic discharges in the brain lead to progressive brain dysfunction. The drug of first choice in the treatment of cognitive epileptic disorders is valproic acid.
Assessment of a child’s mental development includes:
1) pre-speech and speech development; 2) development of perception (ideas about parts of the body, household objects, color, size, shape, orientation in space); 3) memory development (poems, retellings); 4) development of thinking (knowledge about the world around us - time of year, time of day; analytical and synthetic activity, ability to compare, generalize, classify); 5) development of attention (stability, switchability); 6) development of gaming activities; 7) development of visual activities (drawing, modeling) and design (buildings, etc.); development of self-care skills (hygiene skills, neatness, dressing/undressing, eating, etc.); 9) formation of the emotional-volitional sphere (stability of feelings and actions, responsibility, criticality of one’s behavior, self-regulation of behavior); 10) communicative development (contact and adequacy of behavior in communicating with others: the child’s interest in an adult, the ability to attract the attention of an adult, reaction to the adult’s attitude); 11) development of self-awareness (knowledge about oneself - name, surname, address; self-esteem, self-regulation of behavior); 12) development of school skills (counting, reading, writing, etc.).
To study the level of mental development of a child, psychological tests are used (Bayley scale, Denver test and many others). The level of intelligence according to the IQ system is determined in children over 3 years of age.
In ICD-10, mental disorders are discussed in section F80-F89 “Psychological developmental disorders”, and the following main headings are used:
- F80. Specific developmental disorders of speech and language (F80.0. Specific articulation disorder; F80.1. Expressive language disorder; F80.2. Receptive language disorder).
- F81. Specific developmental disorders of learning skills (F81.0. Specific reading disorder (dyslexia); F81.1. Specific spelling disorder (dysgraphia); F81.2. Specific disorder of arithmetic skills (dyscalculia); F81.3. Mixed disorder of learning skills; F81 8. Other disorders of learning skills).
- F82. Specific disorders of the development of motor functions (dyspraxia).
- F83. Mixed specific mental development disorders.
ZPD is often accompanied by conditions reflected in section “F90-F98” of ICD-10 “Emotional disorders and behavioral disorders beginning in childhood and adolescence” (F90. Hyperkinetic disorders: F90.0. Impairment of activity and attention; 90.1. Hyperkinetic behavior disorder ; F91. Behavioral disorders; F93.1. Phobic anxiety disorder; F95. Tics; F98.0. Enuresis of inorganic nature; F98.1. Encopresis of inorganic nature; F98.5. Stuttering, etc.).
The treatment of mental retardation is based on a multidisciplinary approach with the active participation of neurologists, pediatricians, psychologists, psychiatrists, speech therapists, and speech pathologists (including Montessori teachers). The correction must be carried out over a long period of time. The main direction of helping children with mental retardation is a comprehensive psychological and pedagogical correction aimed at improving cognitive development and the emotional-communicative sphere. If it is insufficiently effective, drug therapy is used. In this case, drugs with a nootropic effect (from the Greek noos - thinking, mind, intellect; tropos - turn, direction) become the drugs of choice. According to WHO definition, nootropic drugs are drugs that have a direct activating effect on the central nervous system, improve memory and mental activity, and also increase the brain’s resistance to hypoxia and toxic effects. Their common property is their effect on the higher integrative and cognitive functions of the brain - memory, perception, attention, thinking, speech, emotional-volitional functions. When using vasoprotectors, the nootropic effect develops secondarily, due to the positive effect on cerebral blood flow.
Currently, the following neurotropic drugs are used for mental retardation:
1) pyrrolidone derivatives: piracetam, etc.; 2) pyridoxine derivatives: Biotredin, Encephabol; 3) derivatives and analogues of gamma-aminobutyric acid (GABA): Aminalon, Picamilon, Phenibut, Pantogam; 4) drugs that enhance cholinergic processes: Gliatilin, Ceraxon, Encephabol, Cerebrolysin; 5) glutamatergic drugs: Glycine, Akatinol Memantine; 6) neuropeptides and their analogs: Cerebrolysin, Actovegin, Cortexin, Cerebramin, Semax; 7) cerebrovascular agents (vinpocetine, cinnarizine, Instenon, Ginkgo Biloba, Vasobral, etc.); homeopathic remedies (Cerebrum compositum H, etc.); 9) vitamin-like products (Idebenone, Magne B6, etc.); 10) antihypoxants and antioxidants (Mexidol, Cytoflavin, Encephabol); 11) general tonics (Cogitum, Elkar, Lecithin, etc.); 12) B vitamins (Neuromultivitis, etc.).
The choice of medication is made taking into account the individual characteristics of the child and comorbid conditions. In this case, the leading factor is the excitability of the nervous system. In case of increased excitability of the central nervous system, preference is given to drugs without an stimulating effect (Pantogam, Picamilon, Glycine, Phenibut, Cortexin, Cerebrum compositum, Mexidol, Encephabol, Phezam) or a combination of a nootropic with a sedative (Nervohel, Valerianahel, Lecithin, Magne B6, etc.). In cases where electroencephalography does not reveal epileptiform activity in a patient, a drug from the group of nootropics is selected. It should be noted that in the absence of clarity about the pathogenesis of cognitive impairment, this choice is often random from among numerous drugs, in a large number of cases not having undergone adequate testing for effectiveness. In any case, monotherapy is recommended, prescribed in one or two doses per day.
For delayed psychomotor development in children under one year of age, attention deficit hyperactivity disorder, as well as mental retardation with predominantly speech disorders in preschool children, Encephabol has been effectively used for more than 15 years in Russia. Controlled clinical studies have shown the effectiveness of the nootropic pyritinol (Encephabol).
Encephabol's place among modern nootropics is not entirely usual. According to the formal criteria for the classification of nootropics, Encephabol belongs to a mixed type of drug (neuroprotector) and is included in the subgroup of antioxidants. Indeed, the antioxidant mechanism is one of the leading (but far from the only) in the spectrum of its pharmacological activity. However, if we proceed from the clinical and pharmacological effects of Encephabol, including its influence on intellectual and mnestic functions, then this drug is close to true nootropics (racetam derivatives and cholinergic drugs). This unique effect of Encephabol determines the pharmacological features and indications for clinical use unique to this drug.
Pyritinol (Encephabol) is a double pyridoxine molecule. The active ingredient of Encephabol is pyritinol. In terms of its chemical structure, it is close to pyridoxine (vitamin B6), being essentially its double molecule, but it has slightly different pharmacological effects from pyridoxine.
Pyridoxine (vitamin B6) is a precursor of glutamate and GABA, the main neurotransmitters in the central nervous system, which may be responsible for its nootropic properties. Pyritinol activates brain metabolism, cholinergic transmission, helps stabilize the membrane of nerve cells, prevents the formation of free radicals, which is obviously associated with its neuroprotective properties.
In experiments, it improves the interhemispheric conduction of nerve impulses, corrects prenatal and perinatal disorders of brain development in mice with hyperactivity, learning and coordination disorders. Controlled studies have revealed the possibilities of pharmacotherapy with Encephabol for patients with delayed general and speech development, dysphasia, dyslexia, dysgraphia and disarticulation, and learning difficulties. A study of cognitive electrical potentials of the brain showed that improvement during treatment with pyritinol is due to an increase in the speed and volume of information processed.
The most important aspect of the action of pyritinol is its effect on the energy metabolism of the cell. Under the influence of pyritinol, which perfectly penetrates the blood-brain barrier, the transport of glucose and sodium in neurons is enhanced, as well as the exchange of phosphates between nervous tissue and blood is slowed down [12], and phosphates, the most important substrate for energy supply, accumulate in neurons. In order to assess the significance of this combination of mechanisms of action from the point of view of clinical practice, it should be remembered that the determinant pathological process in cerebral ischemia is not a lack of oxygen (playing only a causal role), but the energy deficiency of Encephabol generated by it is much more diverse in structural and functional terms, than just the effect on the energy supply of neurons.
This drug is directly involved in protein synthetic processes in nerve cells, in particular in the processes of messenger RNA biosynthesis. Perhaps this mechanism plays an important role in the implementation of the mnemotropic effects of Encephabol, its influence on various types of memory, as well as in improving plastic processes in the central nervous system.
It is important to note that the mentioned effects of Encephabol are realized primarily in the limbic-reticular complex. It is obvious that Encephabol, by activating the reticular formation, significantly increases the functional activity of the brain and is a fairly powerful neurodynamics agent.
It is necessary to emphasize the presence of a vascular component in the action of Encephabol. To this day, the question remains debatable to what extent its vasotropic properties are primary (direct impact on metabolic processes in the wall of cerebral vessels), and to what extent secondary, as a result of a normalizing effect on the neurons of the vasomotor centers of the brain. However, under the influence of Encephabol, there is a normalization of blood flow in ischemic regions of the central nervous system, an improvement in microcirculation and rheological properties of blood - an increase in the elasticity of erythrocytes and a decrease in blood viscosity (due to an increase in the ATP content in the erythrocyte membrane).
In the official annotation for Encephabol there are no contraindications for its use in epilepsy, and an analysis of the literature did not reveal any publications on its proconvulsant action in the highwire.stanford.edu database (a total of 162 publications from 1970 to 2010). It is possible to use this drug as an additional drug to antiepileptic therapy to correct cognitive deficits. It has been shown that pyritinol activates glutamate decarboxylase, thereby increasing the production of the inhibitory neurotransmitter GABA, accordingly, the anticonvulsant effect of pyritinol has been shown in experimental epilepsy. The minimal potential for drug-drug interactions of Encephabol makes it possible for its widespread use as part of the complex treatment of epilepsy.
Based on our own many years of experience in using Encephabol, we analyzed the most common clinical effects of Encephabol in the treatment of mental retardation (
).
The most important clinical characteristic of Encephabol is its safety, which is especially important given the specificity of the population - the main consumers of this drug - pediatrics, where safety problems are not inferior in importance to the evaluation of effectiveness. Adverse reactions when taking Encephabol occur rarely and, as a rule, are associated with its general stimulating effect (insomnia, increased excitability, mild forms of dizziness) or, in extremely rare cases, with individual intolerance (allergic reactions, dyspeptic manifestations). All of the above symptoms are almost always transient and do not always require discontinuation of the drug.
On the Russian pharmaceutical market, the drug Encephabol is presented in the form of an oral suspension of 200 ml in a bottle and film-coated tablets of 100 mg.
The dosage of Encephabol is usually, depending on the stage of the pathological process and individual reaction:
- for adults - 1-2 tablets or 1-2 teaspoons of suspension 3 times a day (300-600 mg);
- for newborns - from the 3rd day of life, 1 ml of suspension per day in the morning for a month;
- from the 2nd month of life, the dose should be increased by 1 ml every week to 5 ml (1 teaspoon) per day;
- for children from 1 year to 7 years - 1/2–1 teaspoon of suspension 1–3 times a day;
- for children over 7 years old - 1/2–1 teaspoon of suspension 1–3 times a day or 1–2 tablets 1–3 times a day.
Although the first clinical results of Encephabol may appear after 2-4 weeks of taking the drug, optimal results are usually achieved with a course duration of 6-12 weeks.
Literature
- Amasyants R. A., Amasyants E. A. Clinic of intellectual disorders. Textbook. M.: Pedagogical Society of Russia, 2009. 320 p.
- Current problems in diagnosing mental retardation in children / Ed. K. S. Lebedinskaya. M., 1982.
- Bazhenova O. V. Diagnosis of the mental development of children in the first year of life. M., 1987.
- Bruner J., Olver R., Greenfield P. Studies of cognitive development. M., 1971.
- Burchinsky S.G. Modern nootropic drugs // Journal of a practical doctor. 1996, no. 5, p. 42–45.
- Burchinsky S. G. Ancient brain and age-old pathology: from pharmacology to pharmacotherapy // Bulletin of pharmacology and pharmacy. 2002, No. 1, p. 12–17.
- Voronina T. A., Seredenin S. B. Nootropic drugs, achievements and prospects // Experimental and clinical pharmacology. 1998, no. 4, p. 3–9.
- Voronina T. A. The role of synaptic transmission in memory processes, neurodegeneration and the mechanism of action of neurotropic drugs // Experimental and clinical pharmacology. 2003, No. 2, p. 10–14.
- Dolce A. Review of experimental studies on Encephabol (pyritinol). In the book: Encephabol: aspects of clinical application. M., 2001, p. 43–48.
- Zavadenko N. N. Nootropic drugs in the practice of a pediatrician and child neurologist. M., 2003, 23 p.
- Zozulya T.V., Gracheva T.V. Dynamics and prognosis of the incidence of mental disorders in older people // Journal of Neuropathology and Psychiatry. 2001, v. 101, no. 3, p. 37–41.
- Kovalev G.V. Nootropic drugs. Volgograd, Nizhne-Volzhskoye book. ed., 1990, 368 p.
- Kryzhanovsky G. N. Dysregulation pathology // Dysregulation pathology. 2002, p. 18–78.
- Lebedeva N.V. Encephabol and its analogues in the treatment of neurological diseases. In the book: Encephabol: aspects of clinical application. M., 2001, p. 27–31.
- Lebedeva N.V., Kistenev V.A., Kozlova E.N. et al. Encephabol in the complex treatment of patients with cerebrovascular diseases. In the book: Encephabol: aspects of clinical application. M., 2001, p. 14–18.
- Lebedinsky V.V. Mental development disorders in children. M., 1985.
- Lebedinsky V.V. Disorders of mental development in childhood: Textbook. aid for students psychol. fak. higher textbook establishments. M.: Publishing House, 2003. 144 p.
- Markova E. D., Insarov N. G., Gurskaya N. Z. et al. The role of Encephabol in the treatment of extrapyramidal and cerebellar syndromes of hereditary etiology. In the book: Encephabol: aspects of clinical application. M., 2001., p. 23–26.
- Maslova O.I. Rehabilitation tactics for children with neuropsychic development delays. Russian medical journal. 2000, vol. 8, no. 18, p. 746–748.
- Maslova O.I., Studenikin V.M., Balkanskaya S.V. et al. Cognitive neurology // Russian Pediatric Journal. 2000, No. 5, p. 40–41.
- Mnukhin S.S. About time delays, slow tempo of mental development and mental infantilism in children. L., 1968.
- Notkina N.A. et al. Assessment of the physical and neuropsychic development of children of early and preschool age. St. Petersburg: Detstvo-Press, 2008. 32 p.
- Petelin L. S., Shtok V. N., Pigarov V. A. Encephabol in the neurological clinic // Encephabol: aspects of clinical application. M., 2001, p. 7–11.
- Pshennikova M. G. Stress: regulatory systems and resistance to stress damage // Dysregulation pathology. 2002, p. 307–328.
- Brain aging / Ed. V. V. Frolkis. L., Nauka, 1991, 277 p.
- Amaducci L., Angst J., Bech O. et al. Consensus conference on the methodology of clinical trial of “Nootropics” // Pharmacopsychiatry. 1990, v. 23, p. 171–175.
- Almquist & Wiksell. Scientific studies in mild mental retardation: Epidemiology; a. prevention: Proc. of the 2nd Europe. symp. on scientific studies in Mental Retardation, U Sweden, June 24–26, 1999. - 240 p.
- Bartus R., Deen O., Beer T. Cholinergic hypotheses of memory dysfunction // Science. 1982, v. 217, p. 408–417.
A. P. Skoromets1, 2, 3, Doctor of Medical Sciences, Professor I. L. Semichova4 I. A. Kryukova1, 2, 3, Candidate of Medical Sciences T. V. Fomina6 M. V. Shumilina3, 5 1SPbMAPO, 2SPbGPMA, 3DGB No. 1, 4 St. Petersburg State Center "Child Psychiatry", 5 St. Petersburg State Medical University, St. Petersburg 6 Medical Unit 71 FMBA RF, Chelyabinsk
Contact information for authors for correspondence
Rice. (primary and secondary ZPR), n = 500, age 1–3 years. Encephabol course 8 weeks, 1–2 tsp. per day in the first half of the day
Causes
All causes of mental retardation are divided into two large groups.
Biological
Pathologies and complications during pregnancy:
- if the mother suffered severe toxicosis, infection, intoxication, or injury during pregnancy;
- multiple births;
- intrauterine fetal hypoxia;
- prematurity;
- asphyxia;
- Rhesus conflict;
- incorrect presentation;
- birth injuries.
Infectious, toxic and traumatic diseases leading to perinatal encephalopathy in the first years of a baby’s life:
- nuclear jaundice;
- operations under anesthesia;
- fetal alcohol syndrome;
- cardiovascular pathologies;
- minimal brain dysfunction, organic brain damage, traumatic brain injury;
- congenital visual and hearing impairments;
- low mobility;
- asthenia;
- malnutrition, neuroinfections, influenza, rickets, hydrocephalus, vegetative-vascular dystonia, epilepsy.
Biological reasons also include genetics. There are cases when deviations of this kind are diagnosed from generation to generation.
Social
These include:
- long-term limitation of life activity;
- social deprivation;
- communication deficit;
- unfavorable upbringing conditions;
- mild mental disabilities in parents;
- psychotrauma.
Among the unfavorable conditions of upbringing that lead to mental retardation, there are three most common ones.
Neglect
A child to whom parents do not pay sufficient attention from early childhood, do not engage with him, do not develop him, grows up to be affectively labile, impulsive and suggestible. Does not learn basic rules of behavior and has no intellectual interests. Successful learning requires a basic understanding of the world around us. Reminds me of Mowgli who found himself in civilization. As a result, abnormal personality development is diagnosed as mental instability. But this is not the same as pedagogical neglect.
Overprotection
A child who, from early childhood, is given too much attention by anxious and suspicious parents and is raised as a little “god” of the family. He does not know how to overcome difficulties on his own, or adequately correlate desires and needs with the necessary efforts. There is no willpower. This leads to emotional lability, lack of initiative, self-centeredness, and dependence on adults. As a result, psychogenic infantilism is diagnosed.
Authoritarianism
A child who is suppressed by authoritarian parents from early childhood experiences their aggression, rudeness, cruelty, and despotism. Physical violence is often used. Against such an unfavorable background, obsessions, indecision, phobias, neuroses, increased levels of anxiety, and autism develop. This is an emotionally immature person who is not aimed at achieving success. As a result, learned helplessness syndrome is diagnosed.
How does ZPR differ from ZRR and ZPRR?
Delays in speech and psychospeech development (SRD and DSD) occur as a result of organic lesions of the brain and central nervous system. The reasons for the delay may be: illnesses suffered by the mother during pregnancy, fetal hypoxia, birth pathologies, chromosomal or genetic diseases, severe infections, congenital anomalies of the central nervous system, cerebral vascular pathologies, cerebral palsy, mental illnesses (epilepsy, etc.), tumors brain, etc.
For ZRR and ZPRR:
- intellectual impairments are secondary, and timely correctional work aimed at speech development gives positive dynamics in the normalization of intelligence;
- the lag is not synchronous - speech development lags behind much more than mental development;
- With timely diagnosis and competent correctional work with specialists and at home with parents, the child will be able to catch up with his peers by the senior preschool age.
For ZPR:
- Initially, it is the intellectual development that does not correspond to age, as a result - problems with speech formation;
- there are no specific speech errors, the level of speech development corresponds to the level of development of younger children;
- speech development is delayed as much as general mental development as a whole - synchrony is maintained;
- speech can develop spontaneously, just later than in peers. To correct secondary speech problems, sessions with a speech therapist may be required.
Clinical picture
Parents should be aware of the main symptoms of mental retardation characteristic of a particular age.
1 year
CPR is not diagnosed at 1 year of age. But a number of alarm bells may indicate a tendency towards it:
- Compared to his peers, the baby began to hold his head up, sit up, crawl, turn, stand up, walk, walk late;
- does not hold objects well;
- cannot coordinate movements;
- moves little;
- unemotional.
In this case, it is necessary to take into account the individual developmental characteristics of the baby and, if in doubt, consult a pediatrician or neurologist.
2 years
Deviations are indicated by:
- ignorance of one's own name;
- lack of response to the simplest questions;
- profuse drooling;
- sleep disorders;
- moodiness, tearfulness, irritability, aggression;
- difficulty maintaining attention on a specific subject.
3 years
- Poor vocabulary (no more than 20 words);
- speech defects;
- lack of basic understanding of the surrounding world (cannot name animals, household items, body parts);
- inability to formulate coherent speech;
- difficulty completing basic tasks;
- undeveloped imagination;
- uniformity of actions in the game;
- inability to concentrate;
- fast fatiguability;
- aggressiveness, hysteria.
4 years
At 4 years of age, mental retardation is already clearly diagnosed based on specific symptoms.
Physical:
- weak muscle tone;
- kinetosis;
- urinary disorders;
- headache;
- fatigue, weakness, lethargy, immobility.
Cognitive:
- inability to speak coherently;
- poor vocabulary;
- absent-minded attention;
- poor memory;
- inability to remember information visually or auditorily;
- lack of basic knowledge about the world;
- lack of formation of cognitive motivation.
Social:
- aggressiveness, distrust, wariness towards others;
- isolation, autism, self-absorption;
- reluctance to participate in joint games;
- infantilism;
- mood changes.
It is at the age of 4, with timely recognition of mental retardation, that corrective work must begin. In its absence, all these symptoms only increase and deepen at 5-6 years of age. Secondary signs appear: psychosomatic diseases and internal complexes develop, cognitive abilities deteriorate, and social maladaptation is observed.
At primary school age, mental retardation manifests itself more clearly. Such children differ from their peers in behavior and learning abilities. If parents and kindergarten teachers missed this moment and sent such a child to school, the teacher can no longer help but pay attention to this. He needs to master the minimum standard program, without which he cannot transfer such a student to another class. Therefore, at this stage, a medical-pedagogical commission is organized, a diagnosis is made and psycho-correctional work begins.
Characteristic
The psychological characteristics of a child with mental retardation are compiled according to those mental functions that are impaired in him.
Cognitive abilities
Thinking in children with mental retardation:
- normal level of development of visual and effective thinking;
- for the development of visual-figurative thinking, repeated repetition of the task is necessary;
- unformed skills to carry out analysis and synthesis operations;
- poorly formed verbal and logical thinking.
Correctional classes with children suffering from mental retardation should be aimed at developing thinking taking into account these features. They are able to classify objects according to one characteristic: color or shape, for example. The main thing is to eliminate distractions that significantly reduce performance, patiently repeat the task several times and rely primarily on visual-effective thinking, which is developed in them almost the same way as in their peers. In this regard, they have much better prospects for mastering the material when compared with those who have been diagnosed with mental retardation.
Memory in children with mental retardation:
- unstable;
- unproductive;
- involuntary prevails over voluntary;
- visual prevails over verbal;
- minimal self-control, lack of cognitive activity and motivation when learning and reproducing material;
- inability to use memorization techniques and organize memorization work;
- short-term memory is most affected;
- in the presence of interference, the memorization process practically stops;
- Material learned with great difficulty is quickly forgotten.
All of the above specific features of memory in children with mental retardation must be taken into account by teachers and psychologists when organizing classes and by parents when doing homework. The work should be structured in such a way that the support is involuntary and visual memory, and not voluntary and verbal.
Attention:
- scattered;
- weakened if information is presented verbally;
- unstable;
- reduction in parameters such as volume, selectivity, concentration and distribution.
Correction of attention is aimed at increasing volume and concentration. In classes, distribution and constant switching between different types of activities is necessary. Creative assignments are welcome.
Perception:
- superficial;
- slow process of formation of interanalyzer connections:
- deficits in auditory-visual-motor coordination;
- slow speed of building a single, integral image in a presentation.
Correction of perception is aimed at improving subject-research activities and mastering sensory standards. Games to improve coordination, spatial orientation and develop fine motor skills are welcome.
Speech:
- poor vocabulary;
- impaired sound pronunciation;
- unformed lexical and grammatical structure;
- problems with coherent speech;
- defects of the articulatory apparatus.
To develop speech, classes with a speech therapist are simply necessary. At home, parents need to read and talk more with their child. It is recommended to ensure that he constructs sentences correctly and that his speech is coherent.
Interpersonal communication
The process of interpersonal communication in children with mental retardation is difficult due to the inferiority of the prerequisites necessary for successful socialization:
- low cognitive motivation;
- insufficient speech activity;
- defective speech and mental activity;
- immaturity of many components of speech activity.
Therefore, interpersonal communication is characterized by the following features:
- episodic in nature (they are rarely included in games);
- working and playing alone;
- uncoordinated actions in pairs;
- role-playing game is not a joint activity, since there is practically no communication within it;
- inability to fully and clearly answer questions posed, formulate a question independently, speak out, listen to others, maintain a conversation;
- lack of attachment to anyone.
Children with mental retardation are much more willing to play with those who are younger in age. Often, against the background of failed interpersonal contacts, social phobia develops and serious problems with social adaptation arise.
Emotional-volitional sphere
In children with mental retardation, immaturity of the emotional-volitional sphere is observed. Its manifestations:
- emotional instability;
- lack of independence;
- lability;
- easy suggestibility;
- weakness of willpower;
- self-doubt, low self-esteem;
- causeless worry, increased level of anxiety;
- instant mood changes, contrasting emotions;
- inadequate cheerfulness, gaiety.
Children with mental retardation cannot correctly assess:
- situation: they react too aggressively to any failure and difficulties;
- emotional state of others: during the funeral they can laugh and have fun;
- own emotions.
This is interesting! Children with mental retardation, characterized by emotional immaturity, perfectly recognize emotions from facial expressions and pictures. Compared to their peers, they almost 100% find grimaces of anger, suffering and joy.
Psychological characteristics
A child with mental retardation has features of mental development that differ from the symptoms of other similar pathologies. This is necessary to know to differentiate the diagnosis.
Differences from mental retardation:
- partial rather than complete impairment of cognitive activity;
- high potential for further development;
- It is not the mental functions themselves that suffer, but the prerequisites for intellectual activity (phonemic hearing, speech, attention);
- spasmodic dynamics of mental activity;
- ability to cooperate with adults;
- the presence of emotions in gaming activities;
- a vivid manifestation of emotion;
- often have a knack for drawing.
Differences from pedagogical neglect:
- lack of education and attention from adults is only one of the reasons, while in neglected children it is the only one;
- behavior is caused by deviations in the emotional-volitional sphere and cognitive abilities, and not by problems in moral and legal consciousness;
- are rarely distinguished by deviant behavior and rebellious character;
- know how to interact with adults.
The success of treatment and correction will depend on the correct diagnosis.
Classifications
Classification by Pevzner and Vlasova
M. S. Pevzner - defectologist, psychiatrist, psychologist, candidate of medical sciences and doctor of pedagogical sciences. Professor. T. A. Vlasova is a psychologist, defectologist, Doctor of Psychology, professor, academician. Years: 1972-1973.
- Uncomplicated psychophysical and mental infantilism
The emotional-volitional sphere corresponds to the development of younger children. Playful activity prevails over cognitive activity. This leads to inattention and learning problems.
- Secondary ZPR
The exhaustion of mental functions is caused by various biological factors that occurred during pregnancy or in the first year of the baby’s life.
Lebedinskaya classification
K. S. Lebedinskaya is a child psychiatrist and defectologist. Year: 1982. The basis is the classification of Pevzner and Vlasova, supplemented and expanded.
- Constitutional ZPR
Corresponds to uncomplicated mental and psychophysical infantilism according to the classification of Pevzner and Vlasova. Such children show bright, but superficial and unstable emotions. They are always in a high mood, they are mediocre and naive. They are distinguished by their gracefulness - an infantile body type. ZPR is caused by hereditary factors and complications during pregnancy.
- Somatogenic ZPR
Firstly, it occurs against the background of diseases suffered by the baby in the first year of life. Secondly, it is complicated by neurotic deviations. Such children are not self-confident, fearful, capricious, and feel their physical inferiority. All this ultimately leads to somatogenic infantilism - delayed emotional development.
- Psychogenic mental retardation
The main reason is unfavorable upbringing conditions, starting from a very early age and lasting for a long time.
- Cerebral-organic mental retardation
The most common type of ZPR. I. F. Markovskaya (Candidate of Psychological Sciences, Associate Professor) identifies another mini-classification within this group (1983).
1. Mental instability. Manifests itself in the form of hyperactivity, excessive noise, loudness, rudeness and conflict. But these children’s emotions are short-lived, so within a minute they will be playing with those with whom they just quarreled or even fought.
2. Mental retardation. Such children are dependent, indecisive, timid, slow, and too attached to their parents. They do not participate in joint outdoor games with others, they quickly get lost and cry when something is demanded of them.
Kovalev's classification
V.V. Kovalev - psychologist, psychotherapist. Year - 1979.
This is a classification of mental retardation caused by biological factors:
- dysontogenetic - mental infantilism;
- encephalopathic - organic lesions of the nervous system;
- secondary due to sensory defects - visual and hearing impairments;
- social deprivation - hospitalism.
Today, Lebedinskaya’s classification is most actively used in practice. Although she will soon be 40 years old. In connection with new standards of training and the changed realities of modern life, experts have long been talking about the need to create a more relevant typology of ZPR.
ZPR by type of origin
Below is a table with the causes and symptoms of different types of mental retardation.
| Classification of ZPR | Signs | Causes |
| Constitutional origin | Height, weight and appearance below the age norm, emotional instability, infantilism in various areas | Heredity, pathologies during pregnancy, multiple births |
| Somatogenic origin | Increased anxiety, isolation, lack of communication with others | Somatic diseases suffered at an early age (pathologies of the cardiovascular system, asthma, infections) |
| Psychogenic origin | Lack of social skills, weak psycho-speech factor, timidity, low intellectual and everyday skills, educational lag | Somatic illnesses, upbringing in unfavorable conditions (attention deficit, overprotection or violence) |
| Cerebral-organic origin | Emotional instability, borderline personality type, infantilism manifested in all areas, weak central nervous system | Injuries during childbirth, intoxication of the body, fetal asphyxia, central nervous system diseases |
Diagnostics
The presence of mental retardation in a child can only be confirmed by special diagnostics. Specialists in the field can understand the nature and depth of existing violations during a comprehensive examination:
- psychotherapist;
- speech pathologist;
- psychologist;
- speech therapist;
- pediatrician.
All of them are included in a special medical and pedagogical commission, at which the diagnosis is confirmed or refuted, a final decision is made, and recommendations are given on the further development of the child. In addition to psychological characteristics, they carefully study dynamics (data are provided for the last 2-3 years):
- school performance;
- the nature of errors in mathematics and the Russian language;
- handwriting features;
- state of motor skills;
- pace of activity and many other aspects.
The commission is also provided with the results of a full medical examination and medical history.
Based on the data obtained, a conclusion is made whether the child has mental development delay. But, as mentioned earlier, a medical diagnosis of mental retardation has not been made since 1997. In conclusion, terminology from the following part of ICD-10 is used:
Prevention of mental retardation
Prevention of mental retardation includes, first of all, a responsible approach to pregnancy planning. During the period of bearing a child, the mother should try in every possible way to avoid any negative effects on the fetus.
At an early age, the benefits of preventing infectious and various somatic diseases are undeniable. It is important to provide favorable living conditions for the child. If there is the slightest suspicion that a child is developing psychomotor processes, it is necessary to conduct an examination by specialists and promptly begin work to eliminate the condition.
Education
Where and how can a child with mental retardation study:
- integrated education in secondary schools;
- correctional and developmental education based on a person-centered approach in general educational institutions;
- training in educational institutions of the VII type, where all the features of the educational activities of children with mental retardation are taken into account as much as possible.
In 2015, an important document was approved regulating the education of children with mental retardation in secondary schools. This is the “Adapted basic general education program for primary general education for students with mental retardation.” It is included in the “Special basic general education programs of primary general education of the Federal State Educational Standard”. This system is being implemented in regular educational institutions (not correctional) throughout the Russian Federation from September 1, 2021 in accordance with the Letter of the Ministry of Education and Science of the Russian Federation dated June 7, 2013 “On correctional and inclusive education of children.”
From this moment on, children with mental retardation have every right to study not in a correctional school, but in a regular general education school, together with their normally developing peers. In this case, teachers and parents should take into account the following teaching features:
- they require more attention and individual approach;
- they study according to a separate, simplified program;
- Problems in mastering the material are not due to laziness and negligence, but to inability.
Educational psychologists insist that it is much more productive to send a child with mental retardation to a specialized correctional school or transfer him to home schooling.
Features of behavior at a certain age
Baby
As a rule, children with mental retardation later than others begin to hold their heads up, walk and talk independently. There is also excessive excitability, increased or decreased appetite, insomnia and gastrointestinal diseases.
Preschooler
With pathology, children aged 4–6 years do not understand the rules of most children's games and the norms of behavior in public places. Show excessive, inappropriate emotions and have difficulty communicating.
Schoolboy
Children with mental retardation who have entered the first grade find it difficult to study. They need more time to analyze the information received, especially in conditions that interfere with concentration. They often forget about the goal they are pursuing, are quickly distracted, and cannot concentrate. It is also worth noting that with high mental stress, the child experiences emotional and physical discomfort.
Treatment and correction
Depending on the type of mental retardation and the individual characteristics of the child, specialized specialists develop a correctional and developmental program for the child to study. It includes various blocks that provide an integrated approach to solving existing problems.
Microcurrent reflexology
This is a hardware effect of electrical impulses on bioactive points of the brain, the so-called neuroreflex zones. Targetedly restores the functioning of the nervous system exactly where there are disturbances. Microcurrents selectively process the brain centers responsible for intellectual abilities, speech activity, diction, and vocabulary.
Organized in a hospital setting. True, not all parents give consent to the procedure.
Psychological and pedagogical correctional classes
A child with mental retardation should regularly attend psychologist classes. The goal is to adjust mental development in such a way that it improves his quality of life. Among the main tasks:
- increase the level of intellectual, emotional and social development;
- develop gross and fine motor skills;
- expand your vocabulary and conceptual apparatus.
Parents have the right to know what the program of the psychologist who works with their child includes. Points that raise doubts or mistrust must be agreed upon in advance.
Psychological work with children suffering from mental retardation involves the use of a variety of techniques.
Psychotherapeutic areas:
- isotherapy;
- sand therapy;
- music therapy;
- puppet therapy;
- fairytale therapy;
- logorhythmics;
- methods of object-sensory therapy.
During classes, the psychologist organizes didactic games with multi-colored stripes, cubes, sticks, geometric shapes (including three-dimensional ones) and special cards. Examples of several such games are presented below.
"Guess the Emotion"
It is carried out either in a group of 5-6 similar children with mental retardation, or in pairs with a psychologist. Cards with schematic representations of various emotions are placed on the table. It is proposed to take one of them at random, name what is in the picture, and try to depict this feeling using facial expressions, voice, and gestures. You can make the task more difficult and ask them to name the situation in which this emotion most often manifests itself.
"Find the number"
Pictures and three-dimensional figures of different numbers are laid out on the table. They all differ in size and color. The psychologist names a number - you need to select all the matches from the proposed material (for example, all twos or eights).
"Mood Lotto"
There are cards on the table with animals with different faces on them. The psychologist names an emotion (shows a picture of it or depicts it himself) - the child must choose the right card for it.
"Magic bag"
Small voluminous things that are easily recognizable by touch are put into a beautiful bag: a mirror, an alarm clock, a pencil, a notepad, a ruler, etc. You need to put your hand in there with your eyes closed, take out any object and guess what it is.
"Mood Palette"
There are cards with different shades of mood on the table. The psychologist asks the question: “How do you feel now?” — the child must answer using a drawing. After this, the question is transformed several times: “How is your mother feeling today?”, “What do you think is your cat’s mood?” etc.
Alternative techniques
Additionally, specialized specialists can prescribe modern, non-traditional correction methods:
- hippotherapy;
- canistherapy;
- dolphin therapy;
- feline therapy.
Timely and competently carried out psychocorrectional work gives positive results.
What should parents do?
Psychologists and teachers who work directly with children who have mental retardation give useful recommendations to parents to speed up their development.
To begin with, parents will have to not only understand, but also accept the fact that the child will learn more slowly than his peers and lag behind them in his studies. In order not to demand too much from him, to be patient with his characteristics, they need to be studied and taken into account when communicating and studying.
Homework alone cannot solve the problem of mental retardation. Therefore, the second step for parents who want to help their child is to seek qualified help from specialized specialists - a special education teacher, a psychologist or a psychotherapist. Taking into account individual characteristics, they will give recommendations on what exactly needs to be done.
General tips:
- Exercise daily for 30-40 minutes.
- Pay more attention to the child, organize time together, communicate, involve other relatives.
- Provide a comfortable atmosphere in the family.
- Normalize the daily routine, introduce a healthy lifestyle, provide a balanced diet, increase physical activity and stay in the fresh air.
- Communicate with other parents of the same children (for example, through communities on social networks).
- Organize communication with peers.
- Don't tell your child that he is special. Do not regret that he is not like everyone else.
- Assign household chores, animal care, teach self-care.
- Don't raise your voice, be patient no matter what happens.
- Keep a diary to note all your successes - these entries will help you adjust your future work.